Bilateral Arm Amputation Requires Emergent Vascular Access describes how a teen who suffered a life-threatening accident with a woodchipper, resulting in both arms severed just above the elbow, required emergent and lifesaving vascular access in the Emergency Department of the hospital.
Bilateral Arm Amputation Requires Emergent Vascular Access
– Clinical Case
This case took place in an Emergency Department where a trauma team was working to stabilize a teen patient to prepare him for helicopter transport to a facility with a pediatric specialist that was required to care for this type of medical situation. The teenager had been assisting his family in clearing a wooded area, and one of his gloves got caught in a woodchipper, pulling his arm into the blade. Instinctively, the other arm was used to pull out the first caught arm, and as a result, both arms were involved and were severed just above the elbow. This patient was brought into a trauma room, having suffered massive blood loss. The body responds to massive blood loss by constricting the vasculature – even the largest vessels – to compensate for the drop in blood pressure, which makes obtaining vascular access extremely challenging. Trauma physicians made several unsuccessful attempts at central line placement in the right and then the left jugular vein. They quickly switched to a Femoral approach and were able to obtain access, but the line was positional, meaning it wasn’t stable and completely reliable. Reliable access is critical when patients suffer massive blood loss, which requires immediate fluid resuscitation.
Femoral central lines are a type of central venous catheter device that is inserted into the Femoral vein near the groin or mid-thigh area. Like Internal Jugulars (IJ), they can be a good alternative when other lines are contraindicated or simply not the best choice. Femoral lines are often used in emergency situations when other sites for central line insertion are not available or when a patient requires immediate medical intervention.
Bilateral Arm Amputation Requires Emergent Vascular Access
– Diagnosis and Treatment
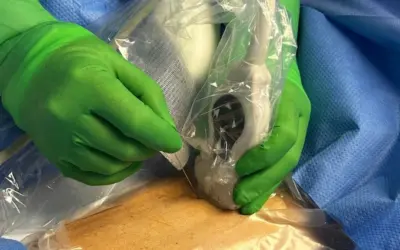
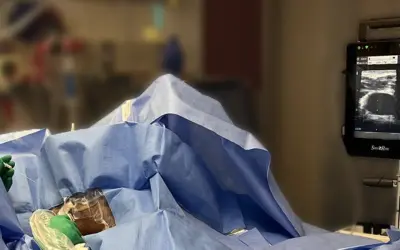
Additional vascular access was urgently needed, and fortunately, a highly skilled and experienced Vascular Wellness clinician was already in the Emergency Department with another patient. Seeing the difficulty in obtaining vascular access and understanding the impact, the charge nurse acted quickly and ran to the Vascular Access-Board Certified (VA-BC) Vascular Wellness nurse clinician and requested her help in the trauma room where the patient was fighting to stay alive. Understanding the dire situation, the Vascular Wellness clinician quickly and successfully inserted an ultrasound guided triple-lumen catheter into the right jugular vein, which was immediately utilized by the team, saving this teenager’s life. The Vascular Wellness nurse clinician suggested an additional central line be placed opposite of the positional left-sided femoral vein inserted by the physicians. The trauma physicians agreed, and this Mid-Thigh Femoral line (similar to the Femoral Line described above but inserted in the mid-thigh area to mitigate risk of infection) was also placed successfully on the first attempt. With two central lines in place, the trauma team was able to stabilize the patient for transport.
During the patient’s three-week stay in the Pediatric ICU recovery unit, he was able to keep the stable central line access until it was no longer needed. The initial trauma team, the transport team, and the receiving critical care team were all thrilled with the expertly placed vascular access in such a challenging and emergent case, allowing them to quickly focus on therapy and the right medications to treat the patient rather than trying to obtain vascular access in order to begin treatment.
Vascular Access Experts
– Key Points
Having a Vascular Access Expert clinician onsite at the time of the patient’s arrival in the trauma unit was fortunate in this frightening situation for the patient and his family. This particular case required rapid critical analysis and vascular access expertise, which can only be accomplished by a highly skilled Vascular Access Expert.
Our team of Vascular Access Experts is responsive, professionally trained, and highly skilled. Our clinician’s expertise often gets utilized successfully after failed attempts by other clinicians. We have a 98+% success rate with 0% insertion-related infection rate across all lines, a three-hour average response time, seven days a week, 365 days a year, and this includes standard and advanced lines which are often placed in challenging cases such as this one and others described in our NCIA case series. We are passionate about advancing healthcare and our commitment to our clients and patients. In this instance, the presence and quick response of the Vascular Access clinician helped save a life. Our clients know our clinicians have the problem-solving skillsets to assist in critical situations, and they do not hesitate to reach out to our team. In return, we provided our clients and patients with the highest level of specialized vascular access care in the region. In this case, the quick action by the charge nurse, combined with our vascular access specialist’s expertise, prevented a critical situation from worsening.
Our Vascular Access Specialists have placed hundreds of thousands of lines, and it is this diverse, aggregate experience that is incorporated into our best practices and methodology. Our experience enables us to assess a situation and patient properly, and if a patient is contraindicated for a specific central line, we can very often find another safe, viable, clinically appropriate option. In addition, our consultative approach with the treating physician allows for a collaborative relationship that results in better patient outcomes, reduced costs, and lives saved.
Nurse Clinicians in Action is a spotlight series highlighting some of the interesting cases that Vascular Wellness clinicians have encountered and participated in treatment. These cases involve challenging situations or intriguing clinical presentations and may involve more than one Vascular Wellness clinician, as our clinicians have the ability to consult each other while in the field, as well as an on-call Clinical Administrator via a HIPAA (Health Insurance Portability and Accountability) compliant communication app. In addition, our extensive training program and diverse client base, including Level 1 Trauma Centers, Short Term Acute Care Hospitals, Long Term Acute Care Hospitals, and Skilled Nursing Facilities, provide our clinicians with a wide array of clinical experience and why we believe our clinicians, as a group, are the most experienced and best trained and supported vascular access clinicians.
If you require Vascular Access or want to learn more, speak to the team at Vascular Wellness today. For the latest articles and insights, follow us on LinkedIn, Facebook, Twitter, YouTube, and Instagram.
Vascular Wellness provides:
(1) Comprehensive vascular access services to North Carolina, South Carolina, and Virginia; and
(2) Customized vascular access services to Tennessee, Georgia, and West Virginia; and
(3) Support vascular access services to Pennsylvania, Ohio, and Kentucky.
Read more Emergent & ICU Patient Cases
Nurse Clinicians in Action stories highlight some of the interesting cases in which Vascular Wellness clinicians have encountered and participated as valuable team members.
Need a Vascular Access Expert?
We have a 98+% success rate with a 0% insertion-related infection rate across all lines, a three-hour average response time, available 7 days a week, 365 days a year.