Numerous IV Medications for Complex Patient describes a case where a facility ordered a vascular access consult for a DIVA patient with End Stage Renal Disease who had several other serious conditions and needed vascular access for administration of numerous IV medications for this complex patient. A consult is a request for Vascular Wellness to arrive and assess the patient and medical history, recommend the clinically appropriate vascular access device, and then place the device after securing consent from the care team.
Numerous IV Medications for Complex Patient
– Clinical Case
A middle-aged patient on hemodialysis was in the hospital ICU with an altered mental status and needed additional vascular access beyond both an existing tunneled hemodialysis catheter to the left femoral vein and 2 peripheral IVs (PIVs) to receive several IV medications and therapies.
Before determining the most appropriate vascular access device to place, the patient’s complex and extensive medical history needed to be considered. The patient was intubated and suffered from ESRD (End Stage Renal Disease), AFib, hypothyroidism, diverticulosis, type 2 diabetes mellitus, multiple metatarsal amputations (bones in the midfoot area), diabetic foot ulcers, COPD (chronic obstructive pulmonary disease), and more.
The care team needed to administer antibiotics, vasopressors, blood products and sedation medication and therapies intravenously, including Rocephin, Dilaudid, Daptomycin, Amiodarone GTT, Levophed, Propofol, Potassium, Synthroid, Iron, Insulin, and Albumin. Because of the quantity and type of medications needed, which included vesicants, the patient needed a central venous catheter (CVC or central line) to safely administer all of these medications and therapies.
Vesicants are harsh medications such as vasopressors (medications that constrict blood vessels), some antibiotics such as vancomycin, and chemotherapy agents. If vesicants leak outside the vein, they are called extravasations and can be dangerous and even cause permanent damage in some scenarios. Vesicants should be administered through a central venous catheter (CVC or central line) whenever possible, particularly if being administered for several days, to minimize the risk of extravasation.
Read more about IV Infiltration and Extravasation prevention and management HERE.
Numerous IV Medications for Complex Patient
– Diagnosis and Treatment
The Vascular Wellness nurse clinician arrived for the consult to determine what type of central line was best for this patient, and the physician noted that the patient was a very difficult IV access (DIVA) patient due to her many conditions, in addition to the complex medical history and numerous IV medications needed, making this a challenging vascular access case.
The vascular access nurse clinician began her medical history review and visual assessment, knowing that the arms were not the best option for a vascular access device. For patients like this one who have kidney disease and renal failure, vein preservation (limiting vascular access and attempts to save veins for future use) is extremely important to ensure safe and viable intravenous sites for current and future therapy, and failed attempts and medications infused in the wrong space can permanently damage a vein.
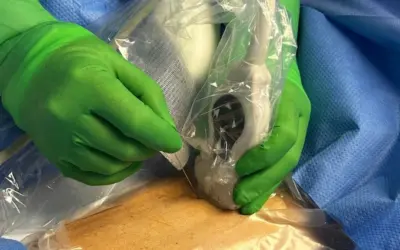
The Vascular Wellness clinician scanned the patient’s left internal jugular (IJ) vein but was unable to visualize it. The patient’s right IJ had multiple marks from previous attempts by the doctors, and as such, was also not a good option. Both axillary veins were too small for cannulation, and the patient’s right leg was very swollen and tight, which indicated it was holding a lot of fluid and made her right femoral vein too deep. Upon evaluation of the left femoral vein, the vascular access clinician determined this was the best option and recommended placing a triple lumen Small Bore CVC in the femoral vein in her mid-thigh, which had an added infection control benefit of being away from the groin area.
The patient’s care team agreed, and the Vascular Wellness nurse clinician began. Although this was a very challenging procedure, especially given the fact the patient’s dialysis catheter was also in this leg, the vascular access nurse expert successfully placed the triple lumen Small Bore device in the mid-thigh on the first attempt.
Several days later, the Vascular Wellness clinician checked in on the patient, and the nursing staff noted that the line was still working perfectly, and they were able to give the patient the medications needed easily and safely.
Vascular Access Experts
– Key Points
As Vascular Access Experts, our clinicians are not only trained and precepted in placing Ultrasound-Guided PIVs, Midlines, and PICCs but they are also trained in placing Small and Large bore advanced central lines. Additionally, our clinicians are highly skilled in identifying contraindications during visual assessments and medical history reviews that take place before any procedure begins. This extensive training and deep skill set, along with bringing to the case all potential supplies needed, enable our clinicians to both help recommend the most clinically appropriate line and then place such line promptly and safely.
The recommendation and ability to place a triple lumen Small Bore Mid-Thigh Femoral line enabled the care team to avoid contraindications associated with chronic kidney disease and preserve the patient’s vasculature in her arms for future needs.
Unlike many of our competitors, our nurse clinicians are hospital credentialed, skill verified semiannually, and Vascular Access Board Certified. They are trained to take all the time needed to perform a comprehensive medical history review to ensure the clinically appropriate line before sticking. It is not unusual for us to collaborate with the medical team and offer recommendations based on the medical history review and treatment plan. These recommendations are often requested by the treating doctors and providers, such as in this case. Through this comprehensive training and focus on the patient and client versus getting to the next procedure, our clients and patients get superior quality at the bedside derived from the hundreds of thousands of lines placed since inception.
Learn more about Vein Preservation and Kidney Disease HERE.
Nurse Clinicians in Action is a spotlight series highlighting some of the interesting cases that Vascular Wellness clinicians have encountered and participated in treatment. These cases involve challenging situations or intriguing clinical presentations and may involve more than one Vascular Wellness clinician, as our clinicians have the ability to consult each other while in the field, as well as an on-call Clinical Administrator via a HIPAA (Health Insurance Portability and Accountability) compliant communication app. In addition, our extensive training program and diverse client base, including Level 1 Trauma Centers, Short Term Acute Care Hospitals, Long Term Acute Care Hospitals, and Skilled Nursing Facilities, provide our clinicians with a wide array of clinical experience and why we believe our clinicians, as a group, are the most experienced and best trained and supported vascular access clinicians.
If you require Vascular Access or want to learn more, speak to the team at Vascular Wellness today.
For the latest articles and insights, follow us on LinkedIn, Facebook, Twitter, YouTube, and Instagram.
Vascular Wellness provides:
(1) Comprehensive vascular access services to Mississippi, North Carolina, Ohio, Oklahoma, Pennsylvania, South Carolina, and Virginia; and
(2) Customized vascular access services to Arkansas, Delaware, Georgia, Tennessee, and West Virginia; and
(3) Support vascular access services to Kentucky.
Read more NCIA Patient Cases
Nurse Clinicians in Action stories highlight some of the interesting cases in which Vascular Wellness clinicians have encountered and participated as valuable team members.
Need an Expert who can Place Central Lines?
We bring skilled, high-quality, timely care to patients in Hospitals, LTACHs, SNFs, Hospital at Home programs, and Outpatient facilities.