Urgent Vascath and Axillary Line describes a critically ill ICU patient in a Trauma Hospital who urgently needed a temporary dialysis catheter for hemodialysis treatment, as she was diagnosed with Diabetic Ketoacidosis (a severe, life-threatening complication with diabetes where the body does not have enough insulin). She was also suffering from sepsis and necrotizing fasciitis due to noncompliance with her wounds.
Urgent Vascath and Axillary Line
– Clinical Case
A Trauma Hospital contacted Vascular Wellness to place a temporary dialysis catheter in a critically ill patient in the ICU. The patient had a medical history of Type 2 diabetes, hypertension, and wounds. The patient was noncompliant and had a current diagnosis of Diabetic Ketoacidosis (DKA), sepsis, and necrotizing fasciitis (a severe, rapidly spreading bacterial infection that destroys soft tissue and muscle fascia) due to noncompliance with her wounds.
The patient had a triple-lumen left side IJ CVC (Internal Jugular central venous catheter, or central line) in place that was infusing vasopressors, sedation medications, fluids, and antibiotics. As such, this Internal Jugular central line was already being used to its maximum capacity.
Urgent Vascath and Axillary Line
– Diagnosis and Treatment
Upon arrival, the Vascular Wellness advanced trained nurse clinician assessed the patient physically and completed a thorough review of the medical history and treatment plan. The patient was noted to have emergent amputations due to necrotizing fasciitis of both lower legs and feet. For this reason, as well as the patient’s body habitus, a Small Bore Mid-Thigh Femoral CVC was not a good option.
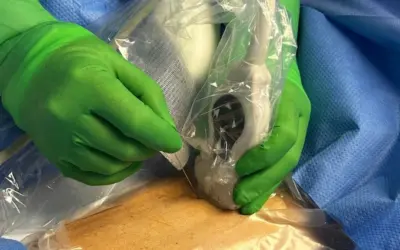
Because the patient already had a triple lumen left side Internal Jugular, the vascular access nurse clinician used the ultrasound to assess the veins on the right side. The patient’s vasculature looked good, and she was able to safely place the Vascath, or temporary dialysis catheter, in the right IJ. The placement was somewhat difficult, but the vascular access nurse clinician had extensive training and experience and was able to place the line on the first attempt.
While the Vascular Wellness nurse clinician was waiting for the chest X-ray confirmation of proper placement so the Vascath could be used, the doctor approached her and requested an additional central line to allow for more access. Once again, the legs were not an ideal option. At this point, both the IJs were being used, and because the patient had renal disease and was still young, it was important to avoid the arms to preserve those veins for possible future fistula sites.
With these considerations and contraindications, the chest was the only other option. There was only one vein large enough in her chest to accommodate vascular access, and that was to use the left axillary vein.
The vascular access nurse clinician once again was able to safely place a triple lumen Small Bore Axillary CVC. Once the patient was stable enough, the left Internal Jugular CVC would be removed to avoid the complications of overcrowding the SVC (superior vena cava) for an extended period of time.
With X-ray confirmation of ideal placement of the Vascath, the patient was able to quickly and safely receive hemodialysis, and the care team had the additional access they needed to try to save the patient’s life.
Urgent Vascath and Axillary Line
– Key Points
As Vascular Access Specialists and Experts, Vascular Wellness pioneered nurse-placed Vascaths. Vascular Wellness’ nurse-placed Vascaths (and Permcaths) at the bedside have many advantages over the primary alternative of physician-placed devices in an Operating Room (OR) or Interventional Radiology (IR) Suite.
Benefits include significantly lower costs, faster hemodialysis treatment, and patient comfort and satisfaction. Physician-placed Vascaths and Permcaths are dependent on OR or IR room and medical personnel availability, so they are typically not able to be performed the same day due to already scheduled procedures. Transportation within a facility or to another facility to get to the OR or IR room is costly and requires significant coordination of resources.
Further, because nurse-placed procedures are at the bedside, only local sedation is needed as compared with physician-placed dialysis catheters that require patients to fast prior to their procedure because of the need for anesthesia, which can cause additional delays in treatment. The use of anesthesia for surgical procedures in an OR adds significant resources and costs for the facility, as well. All of these moving parts can cause Delay Cascades (see References below) for the patient, which are unnecessary delays in receiving essential critical care therapies, particularly in severely ill patients such as the one in this case.
In addition, Vascular Wellness provides our client partners with a dedicated professional team of vascular access experts and specialists who are trained, precepted, and certified in the placement of standard and advanced lines at the patient’s bedside. We promote teamwork, internally and externally, by either becoming an extension of a client’s in-house team or operating as a client’s outsourced provider, and all of our services are customized to meet our clients’ needs. Our deep expertise and collaborative approach have earned us the role as a trusted part of the care team, and with respect to vascular access, we function as a bridge among all stakeholders, such as the patient, their family members, and the providers and staff.
References regarding “Delay Cascade”
1. Heart & Lung. Volume 49, Issue 3, Page 273-286, May-June 2020
2. Journal of Infusion Nursing. 43(4): p222-228, July-August 2020
3. Journal of the American College of Emergency Physicians Open. 2020 Dec; 1(6): 1660–1668
Nurse Clinicians in Action is a spotlight series highlighting some of the interesting cases that Vascular Wellness clinicians have encountered and participated in treatment. These cases involve challenging situations or intriguing clinical presentations and may involve more than one Vascular Wellness clinician, as our clinicians have the ability to consult each other while in the field, as well as an on-call Clinical Administrator via a HIPAA (Health Insurance Portability and Accountability) compliant communication app. In addition, our extensive training program and diverse client base, including Level 1 Trauma Centers, Short Term Acute Care Hospitals, Long Term Acute Care Hospitals, and Skilled Nursing Facilities, provide our clinicians with a wide array of clinical experience and why we believe our clinicians, as a group, are the most experienced and best trained and supported vascular access clinicians.
If you require Vascular Access or want to learn more, speak to the team at Vascular Wellness today.
For the latest articles and insights, follow us on LinkedIn, Facebook, Twitter, YouTube, and Instagram.
Vascular Wellness provides:
(1) Comprehensive vascular access services to Mississippi, North Carolina, Ohio, Oklahoma, Pennsylvania, South Carolina, and Virginia; and
(2) Customized vascular access services to Arkansas, Delaware, Georgia, Tennessee, and West Virginia; and
(3) Support vascular access services to Kentucky.
Read more NCIA Patient Cases
Nurse Clinicians in Action stories highlight some of the interesting cases in which Vascular Wellness clinicians have encountered and participated as valuable team members.
Need an Expert who can Place Central Lines?
We bring skilled, high-quality, timely care to patients in Hospitals, LTACHs, SNFs, Hospital at Home programs, and Outpatient facilities.