Mastectomy and PICC Line can be Unsafe Combination describes how the Vascular Access clinician consulted with the patient’s physician to revise the physician’s order from a PICC Line to the more clinically appropriate Internal Jugular (IJ) Line and is the focus of this Nurse Clinicians in Action.
Mastectomy and PICC Line can be Unsafe Combination
– Clinical Case
This case took place in a hospital with a female patient who had a bilateral mastectomy with lymph node removal within the past year. The managing physician ordered a consult with the Vascular Wellness clinician and a PICC line for the patient as she needed two antibiotics as well as Total Parenteral Nutrition (TPN), a way to bypass the gastrointestinal tract by providing nutrition directly into the vein. Multi-Lumen access was necessary to administer both the antibiotics and the TPN.
Mastectomy and PICC Line can be Unsafe Combination
– Diagnosis and Treatment
After a thorough assessment of the patient including medical records, the Vascular Wellness clinician explained to the managing physician that the patient’s bilateral mastectomy with lymph node removal was contraindicated for having a line placed in the arm as that could lead to lymphedema now or in the future. The Vascular Wellness clinician recommended that a Small Bore Internal Jugular (IJ) line be placed as that was the safest option and the managing physician agreed.
As both the patient and her family were very hesitant, scared, and nervous to have a line placed in the patient’s neck, both the Vascular Wellness clinician and the managing physician were able to explain the process for placement and the importance of using this line over any line placed in the arms as that could lead to side effects. The patient’s fears were allayed, and she agreed to the IJ placement.
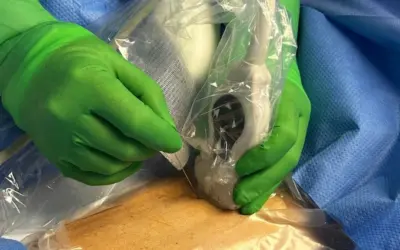
The patient was very pleasantly surprised with the rapidness, efficiency, and comfortability of the procedure. The clinician believes that with the placement of this Small Bore IJ line, this patient was able to receive everything she needed to heal in the safest way possible as well as saving her from a possible large central venous catheter (CVC) in her neck or groin, as well as several possible unsafe punctures in those areas or her arms.
Vascular Access Experts
– Key Points
Vascular Wellness follows best practices from both the Infusion Nurse Society and Association for Vascular Access for patients including those that have survived breast cancer and lymph node removal. A patient who has had a mastectomy with lymph node removal will be contraindicated for PICCs and Midlines on whatever side the lymph nodes were removed. Lymph node removal results in fewer lymph nodes to filter the lymph, a clear fluid that filters waste throughout the tissues in the body. The waste builds up and can lead to lymphedema, an upper extremity swelling that will be permanent. In the case of a bilateral mastectomy, an IJ or Femoral (Fem) line should be used, as they are away from the mastectomy site, reducing the risk of lymphedema.
Vascular Wellness clinicians have placed hundreds of thousands of lines and this experience enables us to assess a situation and patient properly and if a patient is contraindicated for a specific central line, to utilize that experience to place a clinically appropriate line. Further, by having the tools of US Guided PIVs, Midlines, PICCs, Small Bore lines such as Internal Jugular lines (IJs) and Femoral lines (Fems), and Large Bore lines including Vas Caths and Quad Lumens, Vascular Wellness is able to create clinically appropriate access in virtually all patients, while minimizing multiple needle sticks. The ability to minimize sticks and place the right line at the right time, the first time, is incredibly important as the placement of a Central Venous Catheter is an invasive medical procedure that comes with risks. These factors, along with a consultative approach with the treating physician, are just a few reasons why Vascular Wellness improves patient outcomes, reduces costs, and strengthens infection control.
Nurse Clinicians in Action is a spotlight series highlighting some of the interesting cases that Vascular Wellness clinicians have encountered and participated in treatment. These cases involve challenging situations or intriguing clinical presentations and may involve more than one Vascular Wellness clinician, as our clinicians have the ability to consult each other while in the field, as well as an on-call Clinical Administrator via a HIPAA (Health Insurance Portability and Accountability) compliant communication app. In addition, our extensive training program and diverse client base, including Level 1 Trauma Centers, Short Term Acute Care Hospitals, Long Term Acute Care Hospitals, and Skilled Nursing Facilities, provide our clinicians with a wide array of clinical experience and why we believe our clinicians, as a group, are the most experienced and best trained and supported vascular access clinicians.
If you require Vascular Access or want to learn more, speak to the team at Vascular Wellness today.
For the latest articles and insights, follow us on LinkedIn, Facebook, Twitter, YouTube, and Instagram.
Vascular Wellness provides:
(1) Comprehensive vascular access services to Mississippi, North Carolina, Ohio, Oklahoma, Pennsylvania, South Carolina, and Virginia; and
(2) Customized vascular access services to Arkansas, Delaware, Georgia, Tennessee, and West Virginia; and
(3) Support vascular access services to Kentucky.
Learn more about our Vascular Access Solutions
Vascular Wellness provides comprehensive Vascular Access Solutions and Services at the bedside for virtually all healthcare settings.
Need more than just a PICC Service?
We offer timely, innovative, and advanced vascular access services at the bedside, with full administrative support, from skilled employees who care.